Treating a chronic disease as a course: the case for long-term GLP-1 therapy in obesity
GLP-1 receptor agonists lower the body's defended weight range only for as long as they are taken, which makes obesity a chronic disease and these drugs maintenance therapies. Treating them as a weight-loss course with an end date is the central error in how they are used. Correcting it means titrating to durability rather than to a maximal dose, protecting muscle, and closing the persistence and dosing gap that separates real-world results from the trials.
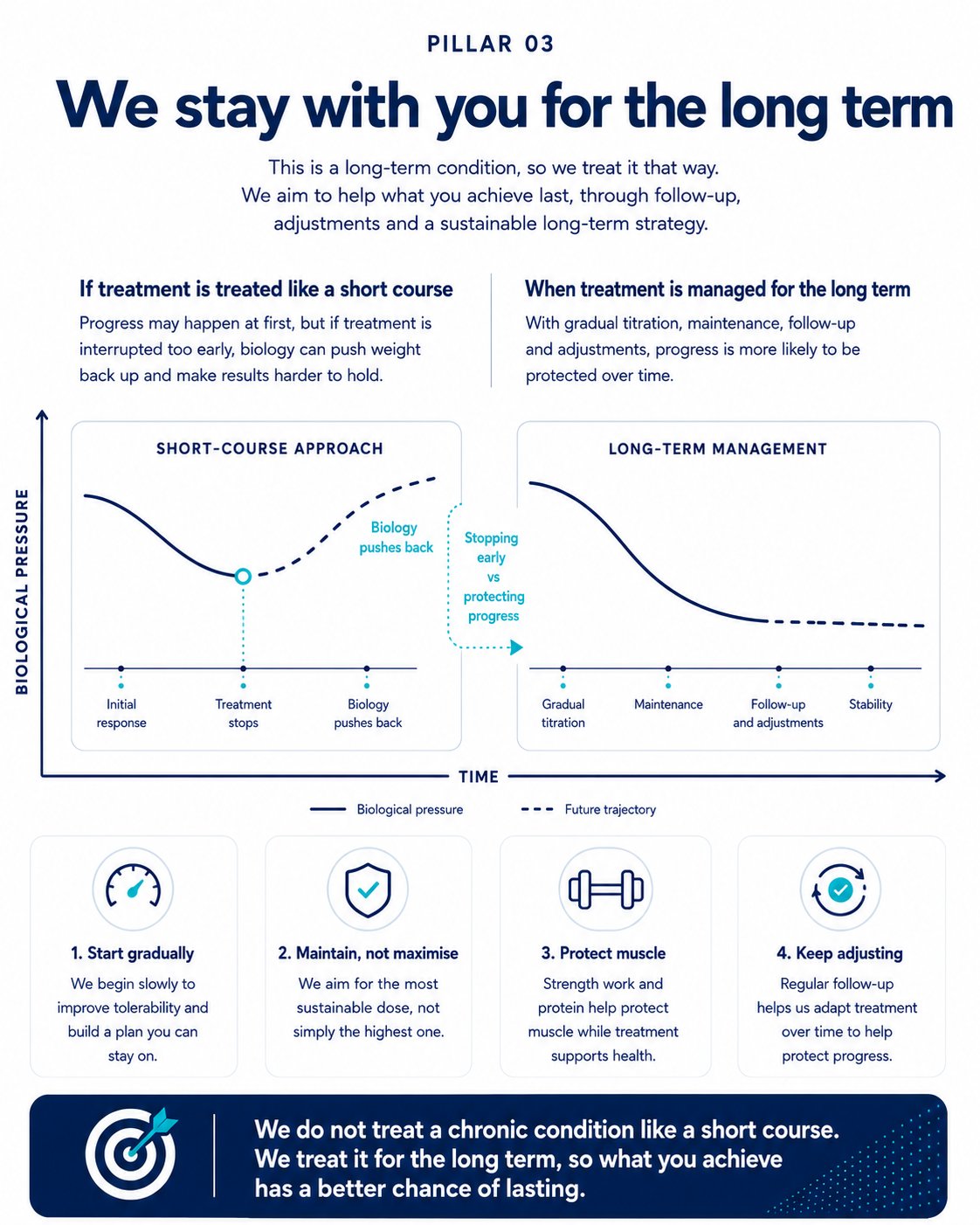
Stopping early vs protecting progress. Long-term management keeps the defended range lower; a short-course approach allows biology to push it back up.
The conclusion the biology forces
Obesity is a defended, multi-system disease in which the body maintains a weight range through the hormonal control of appetite, so that behaviour can move a person within the range while only medicine lowers it. That defended range is the reason these therapies work, and also the reason they cannot be stopped without consequence. When semaglutide was withdrawn at the end of the STEP 1 trial, participants regained around two-thirds of the weight they had lost within a year, and in SURMOUNT-4 those switched from tirzepatide to placebo regained substantially while those who continued maintained their loss. This is not a flaw in the medicines but the predictable behaviour of a homeostatic system whose range has been held lower by treatment rather than reset, as the settling-point models describe, and whose metabolic and hormonal defence of weight persists for years.
The conclusion is unavoidable: obesity is a chronic, relapsing disease, and the drugs that treat it are maintenance therapies. The World Health Organization's first guideline on these agents frames it in exactly these terms and recommends that treatment be planned for the long term, consistent with the clinical definition of obesity. The mental model is familiar everywhere else in chronic disease medicine. No clinician stops a statin when the cholesterol falls, because the normal value is the treatment working rather than the disease resolving, and a normal weight achieved on treatment is the defended range held lower, not the biology cured. The persistent framing of these drugs as a weight-loss course with a beginning and an end is the central error in how they are used.
Not a race to the highest dose
If the aim is maintenance rather than maximal loss, the instinct to escalate every patient to the highest tolerated dose is misplaced. The titration schedules exist for good clinical reasons, because starting low and increasing slowly reduces the gastrointestinal effects that are the commonest reason patients abandon treatment early, and a patient who tolerates a lower dose and remains on it will do better over time than one escalated quickly to a dose they cannot sustain. The objective of long-term treatment is the lowest effective dose that holds the range, not the highest the patient can bear, and for many people durable maintenance is achieved below the maximum studied. This is the posture long-term care requires: titrate to tolerability and durability, maintain rather than maximise, and treat the percentage lost as a means to health rather than as the endpoint itself.
The persistence and dosing gap
The figures that define these medicines in the public mind come from trials conducted under near-ideal conditions, with selected participants, intensive support, regular follow-up and high doses sustained by completion rates of around eighty-five per cent. Real-world practice differs, and its results differ accordingly. Depending on how discontinuation is defined and on insurance and indication, between roughly a third and four-fifths of patients stop within a year, with several large datasets placing the figure around or above half within twelve months. Persistence has improved, reaching roughly sixty per cent at one year in recent commercially insured cohorts against around forty per cent a few years earlier, but it falls steeply thereafter, with only about one in seven patients still treated at three years. The weight outcomes follow. Patients who remain on treatment lose on average close to twelve per cent of body weight, those who stop within three months lose only around three to four per cent, and achieving a ten per cent reduction is associated with remaining on treatment, a higher dose, and tirzepatide rather than semaglutide, while a large proportion never reach or sustain an effective maintenance dose.
The interpretation matters, because the gap is easily read as evidence that the drugs underperform. They do not. The trials describe what the medicine can do; the real-world figures describe what happens when treatment is begun without the support and sustained dosing that make it work and is then stopped early, most often for cost or side effects rather than because the patient no longer needs it. The gap is therefore one of persistence and dosing, and it is one that better long-term care can close.
Reading the real-world discontinuation data correctly
A recent and widely reported analysis complicates this picture in a way that is easily misread. A Cleveland Clinic study of nearly eight thousand patients found that, unlike the controlled withdrawal trials, the average regain after stopping was small, with the obesity group regaining only around half a per cent over the following year and forty-five per cent maintaining or continuing to lose. Taken alone this might seem to license stopping once a target is reached, but the authors' own explanation shows that it does not. The real-world patients had lost considerably less before stopping than trial participants do, on average around eight per cent rather than the fifteen to twenty of the pivotal trials, and smaller losses are inherently easier to maintain; moreover many of those who stopped did not truly cease treating the disease, but restarted the drug, switched to another, or intensified lifestyle support. Read correctly, the finding argues for sustained, individualised management rather than for the course-with-an-end model it is sometimes taken to support.
Protecting muscle
A legitimate concern about rapid and substantial weight loss is that some of what is lost is lean tissue, including muscle, and it should be addressed accurately rather than dismissed. Body composition studies indicate that between a quarter and around two-fifths of the weight lost on these therapies is fat-free mass, with the proportion generally lower for tirzepatide than for semaglutide, and that relative lean mass is usually preserved or improved because fat is lost preferentially. The loss of muscle is substantially modifiable: resistance exercise and an adequate protein intake, in the region of 1.2 to 2.0 grams per kilogram per day, protect lean mass during treatment, and measures of function such as grip strength can improve rather than decline. Long-term treatment done well includes muscle as a deliberate target of care, addressed through exercise and nutrition rather than through dose reduction, because the answer to losing lean tissue is to protect it, not to treat the disease less effectively.
The cascade of thriving
The reason long-term treatment is worth the difficulty it entails is that its benefits extend well beyond the scale and accrue over time in a way a short course cannot. In the SELECT trial, semaglutide reduced major adverse cardiovascular events by about twenty per cent in patients with established cardiovascular disease, and both the weight loss and the benefit were sustained across four years of continued treatment. Sustained treatment also reverses much of the metabolic disease that excess adiposity drives, with a majority of patients with prediabetes returning to normal glucose regulation within a year in real-world cohorts, and beyond the measurable endpoints lie improvements in sleep, mobility, mood and the capacity to do more.
This is the cascade the argument has been building towards. Effective treatment produces durable results, durable results sustain motivation, sustained motivation supports the habits that protect muscle and metabolic health, and the gains beyond weight feed back into continued engagement. Long-term treatment keeps that cycle turning, whereas a course with an end date allows it to collapse back into regain and discouragement; sustained treatment lets a person move from losing weight to living better.
The difficulties, and the goal
A case for lifelong treatment must confront its objections honestly. The first is cost and access, because treating a highly prevalent chronic disease with an expensive medicine indefinitely raises questions of affordability that no clinical argument dissolves, and the burden falls unequally, since people in lower-income groups are both less likely to be prescribed these drugs and more likely to discontinue them, with cost the dominant reason, so that a treatment capable of reducing a disease that tracks deprivation risks widening the inequality it could narrow. The second is long-term safety, because these medicines have been used at scale for a relatively short time, and while the data so far are reassuring, honesty requires acknowledging that we have years rather than decades of population experience and a corresponding obligation of continued surveillance. The third is that lifelong treatment, and a maximal dose, are not necessary for everyone, since some patients maintain at a lower dose and some hold the lower part of their range with lifestyle and return to medication when needed, so that both under-treatment, the current default, and over-treatment are failures of individualised care. None of these makes the disease acute; a chronic condition is not transformed by the inconvenience of treating it for life.
Implications
Treating obesity as the chronic disease it is means diagnosing it clinically rather than by body mass index alone, titrating treatment to tolerability and durability rather than to a maximal dose, protecting muscle through exercise and nutrition, keeping patients in adequately dosed treatment through the support and follow-up that real-world persistence so plainly requires, individualising the intensity and duration rather than applying a single template, and judging success by health rather than by appearance. The prize for doing this well is not merely a lower weight but a longer and better life, available to a person treated for the disease they actually have, in the way that disease actually demands.
- Wilding JPH, Batterham RL, Davies M, et al. Weight regain and cardiometabolic effects after withdrawal of semaglutide: the STEP 1 trial extension. Diabetes Obes Metab. 2022;24(8):1553-1564.
- Aronne LJ, Sattar N, Horn DB, et al. Continued treatment with tirzepatide for maintenance of weight reduction in adults with obesity: the SURMOUNT-4 randomized clinical trial. JAMA. 2024;331(1):38-48.
- Leibel RL, Rosenbaum M, Hirsch J. Changes in energy expenditure resulting from altered body weight. N Engl J Med. 1995;332(10):621-628.
- Sumithran P, Prendergast LA, Delbridge E, et al. Long-term persistence of hormonal adaptations to weight loss. N Engl J Med. 2011;365(17):1597-1604.
- Speakman JR, Levitsky DA, Allison DB, et al. Set points, settling points and some alternative models. Dis Model Mech. 2011;4(6):733-745.
- Fothergill E, Guo J, Howard L, et al. Persistent metabolic adaptation 6 years after The Biggest Loser competition. Obesity (Silver Spring). 2016;24(8):1612-1619.
- World Health Organization. WHO issues its first guideline on the use of GLP-1 receptor agonists for obesity in adults. Geneva: WHO; 2025.
- Rubino F, Cummings DE, Eckel RH, et al. Definition and diagnostic criteria of clinical obesity. Lancet Diabetes Endocrinol. 2025;13(3):221-262.
- Prime Therapeutics. Real-world persistence with GLP-1 therapy for the treatment of obesity. Eagan (MN): Prime Therapeutics; 2024.
- Gasoyan H, et al. Real-world weight reduction with semaglutide and tirzepatide by treatment persistence and dose: a Cleveland Clinic cohort. 2025.
- Gasoyan H, et al. Weight change after discontinuation of semaglutide or tirzepatide: a real-world cohort study. Diabetes Obes Metab. 2026.
- Wilding JPH, Batterham RL, Calanna S, et al. Once-weekly semaglutide in adults with overweight or obesity. N Engl J Med. 2021;384(11):989-1002.
- Jastreboff AM, Aronne LJ, Ahmad NN, et al. Tirzepatide once weekly for the treatment of obesity. N Engl J Med. 2022;387(3):205-216.
- Neeland IJ, Linge J, Birkenfeld AL. Changes in lean body mass with incretin-based therapies for obesity and strategies for mitigation. Diabetes Obes Metab. 2024;26(Suppl 4):16-27.
- Lincoff AM, Brown-Frandsen K, Colhoun HM, et al. Semaglutide and cardiovascular outcomes in obesity without diabetes. N Engl J Med. 2023;389(24):2221-2232.
Competing interests: AA is Medical Director (International) at HeliosX, which provides GLP-1 receptor agonist therapies for weight management. The views expressed are the author's own.