Modifiable, but with medicine: obesity belongs in a third category of risk factor
Risk factors are taught as modifiable or non-modifiable, and obesity is filed among the modifiable, which licenses the assumption that a patient who stays heavy has not tried hard enough. Body weight is defended within an untreated range that behaviour can move a person within but only medicine can lower, by shifting it to a lower treated range. Recognising obesity as modifiable specifically with medical treatment is a distinction with direct consequences for how patients are diagnosed, treated and judged.
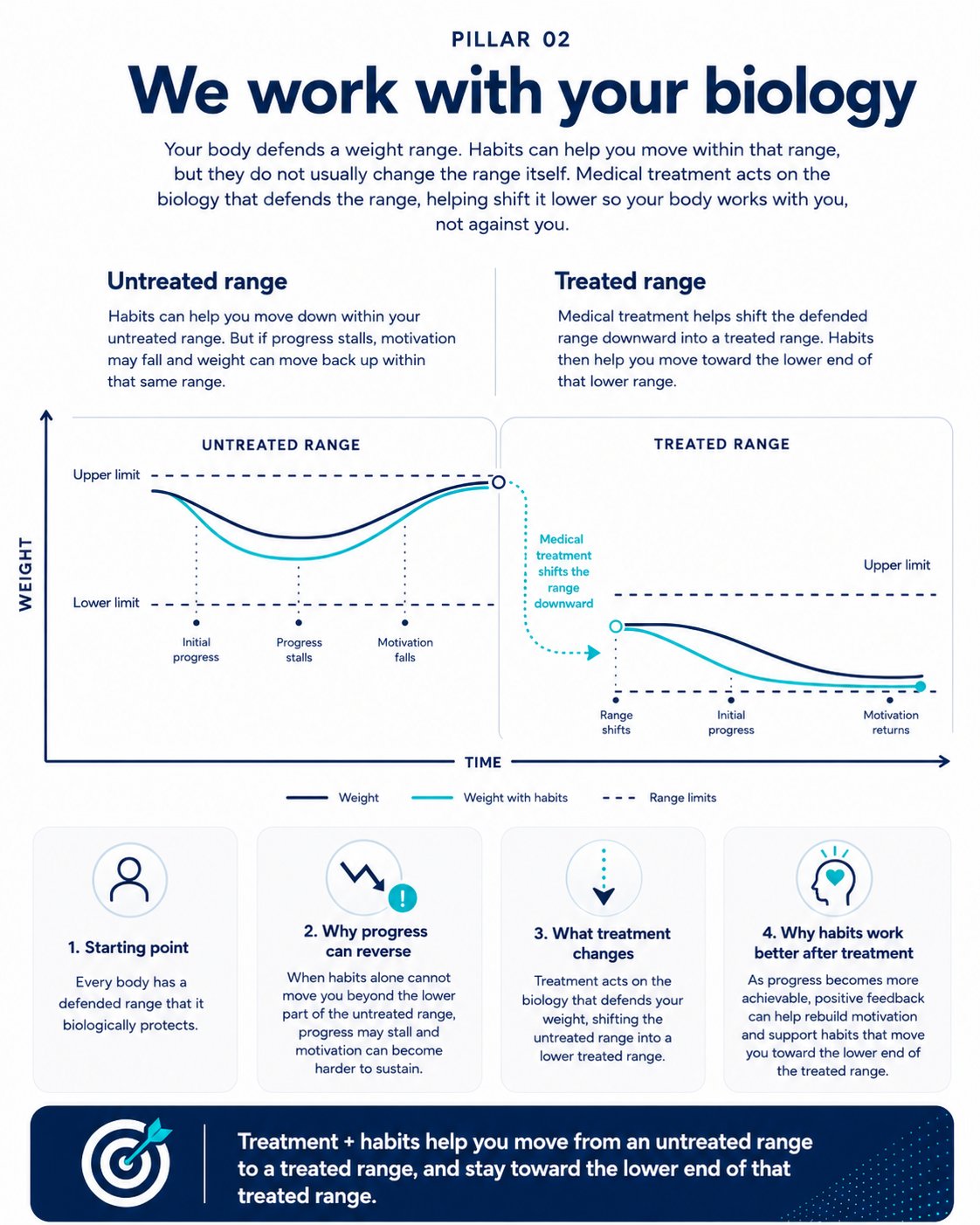
Behaviour moves a person within the untreated range. Medicine shifts that range down to a treated range. Lowering the range changes hard outcomes.
The category problem
Medicine teaches risk factors as two kinds. There are those that cannot be modified, such as age, sex, genetic background and family history, and those that can, such as blood pressure, lipids, glycaemia, smoking, diet, physical activity and body weight. The division is useful, because it directs effort towards what can be changed. The difficulty is the place weight occupies within it. To list weight among the modifiable factors, beside smoking and diet, implies that the means of changing it are the patient's to deploy in the way that stopping smoking or eating differently ostensibly are. From that implication it is a short step to reading a patient who remains heavy as one who has not done the work, and obesity comes to be managed with advice and disappointment rather than with treatment. Yet weight is not modifiable in that sense. It is a heritable, multi-system disease in which the body defends a weight range through the hormonal control of appetite, so that hunger and fullness are regulated outputs rather than expressions of resolve. The question of modifiability cannot be settled by appeal to effort. It can be settled only by asking what actually moves a defended range, and the answer separates cleanly into what behaviour achieves and what medicine achieves.
The ceiling of effort
Consider first what lifestyle change alone delivers, measured over time rather than at the peak of a programme. The most rigorous test remains the Look AHEAD trial, which randomised more than five thousand adults with type 2 diabetes to an intensive lifestyle intervention or usual care. The intervention achieved a weight loss of about 8.6 per cent at one year, better than most real-world programmes, but this eroded to roughly 6 per cent over the longer term, and the trial was stopped early for futility because, despite sustained modest loss and real gains in fitness, it did not reduce cardiovascular events. A meta-analysis of structured programmes found only around 3 per cent of body weight sustained in the long term. The pattern is exactly what defended-weight physiology predicts. Effort moves a person towards the lower part of their untreated range, and the body resists further descent through metabolic and hormonal adaptation. The ceiling is the height of the wall the biology builds, not a failure of the people who run up against it. This does not make lifestyle worthless, and the point should not be mistaken for that. Diet, activity and sleep improve cardiometabolic health, protect fitness and reduce risk by routes that have nothing to do with the scale. As a lever on the defended weight itself, however, behaviour tops out at a few per cent, and additional resolve does not raise the ceiling, because the resistance is physiological.
The reach of medicine
Set against that ceiling, the effect of medical treatment is categorical rather than incremental. In STEP 1, once-weekly semaglutide produced a mean loss of about 14.9 per cent against 2.4 per cent on placebo, and in SURMOUNT-1, tirzepatide produced losses of up to roughly 22.5 per cent at the highest dose, several times the lifestyle ceiling and achieved by acting on the same central appetite circuits that defend weight. The decisive evidence is the consequence rather than the magnitude. In SELECT, conducted in more than seventeen thousand adults with established cardiovascular disease and overweight or obesity but without diabetes, semaglutide reduced major adverse cardiovascular events by about 20 per cent. Where intensive lifestyle intervention tested at scale did not move cardiovascular endpoints, medicine did.
The contingency of the effect confirms the mechanism rather than undermining it. The STEP 1 extension found that about two-thirds of lost weight returned within a year of stopping, and SURMOUNT-4 showed that those continuing treatment maintained their loss while those switched to placebo regained. Withdrawal returns weight because the range, defended by the metabolic and hormonal adaptations to weight loss, is held in its lower treated state by treatment rather than re-set, and returns toward the untreated range when treatment stops. Behaviour moves a person within the untreated range; medicine shifts that range down to a treated range; and lowering the range changes hard outcomes.
A third category
If behaviour cannot lower the untreated range and medicine can, then weight does not behave like the other factors in the modifiable column, and the framework needs a more accurate place for it. It is not non-modifiable, since with treatment it has become one of the most modifiable risk factors in clinical medicine, more responsive in the scale of achievable change than blood pressure or lipids. Yet it is not modifiable by the patient's effort in the way the column implies. The precise description is a third tier between the two we inherited: non-modifiable, lifestyle-modifiable and medically modifiable. Age and genotype occupy the first; blood pressure, lipids and glycaemia straddle the second and the third; obesity, on current evidence, belongs in the third, a risk factor effectively immovable until medicine made it movable and movable principally through medical treatment.
Naming it matters for two reasons. The first is precision, because the label tells the clinician where the effective lever lies and so guards against the long detour of escalating advice in the hope that more of what reaches a few per cent will somehow reach fifteen. The second is attribution, because a condition in the medically modifiable tier is one a clinician treats, not one a patient is reproached for having. The category removes the patient from the dock, and it does so without lowering clinical standards.
The cost of getting it wrong
Miscategorisation is not inert, and its costs are measurable. Perceived weight discrimination is associated in large longitudinal studies with an increased likelihood of becoming and of remaining obese, and weight stigma drives disordered eating, avoidance of physical activity and avoidance of healthcare itself. The wrong category is self-reinforcing: it blames the patient, the blame drives disengagement, and disengagement worsens the very outcome. Correct categorisation runs the process in reverse, because to tell a patient that their weight is a medically modifiable condition rather than a personal failing is itself a clinical act that re-engages, and re-engagement is the entry point to a reinforcing cycle in which treatment lowers the range, the results are durable, motivation is sustained because effort is finally rewarded, and the benefits extend beyond weight to fitness, sleep, mood and a recovered sense of agency.
There is precedent for such a reclassification. For most of the twentieth century, peptic ulcer disease was attributed to stress and diet and managed with advice to live more calmly, until Marshall and Warren identified Helicobacter pylori in 1984 and the disease became a bacterial infection cured by antibiotics. A population dimension reinforces the point: the food environment shifts the weight a whole population defends, and obesity tracks deprivation closely, a pattern inconsistent with a sudden and uneven collapse of individual willpower.
What the category does not claim, and what follows
The case is easy to overstate in ways that would discredit it, and its limits should be stated plainly. It does not claim that everyone with obesity needs medication, since thresholds, comorbidity, preference, tolerability and access all bear on the decision, and the category describes where the lever lies rather than mandating that it be pulled in every case. It does not retire lifestyle, which remains necessary, protects lean mass alongside pharmacological treatment and reduces risk by routes other than weight; the relationship is both and, not either or. Its real hazard is over-medicalisation, the reframing of every elevated body mass index as a prescription waiting to be written, which is precisely why the category must be tethered to a clinical definition of disease requiring adiposity together with impairment, and not to the number alone.
The category also presses the next question into view. If the range is lowered to a treated state only while treatment continues, then obesity is a chronic condition requiring long-term management rather than a course of treatment with an end date, the position taken by the World Health Organization's first guideline on these therapies and consistent with the clinical definition of obesity that anchors this argument. How that long-term treatment is done well, and what it asks of patients and clinicians, is the question that remains.
- Look AHEAD Research Group; Wing RR, Bolin P, Brancati FL, et al. Cardiovascular effects of intensive lifestyle intervention in type 2 diabetes. N Engl J Med. 2013;369(2):145-154.
- Anderson JW, Konz EC, Frederich RC, Wood CL. Long-term weight-loss maintenance: a meta-analysis of US studies. Am J Clin Nutr. 2001;74(5):579-584.
- Wilding JPH, Batterham RL, Calanna S, et al. Once-weekly semaglutide in adults with overweight or obesity. N Engl J Med. 2021;384(11):989-1002.
- Jastreboff AM, Aronne LJ, Ahmad NN, et al. Tirzepatide once weekly for the treatment of obesity. N Engl J Med. 2022;387(3):205-216.
- Lincoff AM, Brown-Frandsen K, Colhoun HM, et al. Semaglutide and cardiovascular outcomes in obesity without diabetes. N Engl J Med. 2023;389(24):2221-2232.
- Wilding JPH, Batterham RL, Davies M, et al. Weight regain and cardiometabolic effects after withdrawal of semaglutide: the STEP 1 trial extension. Diabetes Obes Metab. 2022;24(8):1553-1564.
- Aronne LJ, Sattar N, Horn DB, et al. Continued treatment with tirzepatide for maintenance of weight reduction in adults with obesity: the SURMOUNT-4 randomized clinical trial. JAMA. 2024;331(1):38-48.
- Leibel RL, Rosenbaum M, Hirsch J. Changes in energy expenditure resulting from altered body weight. N Engl J Med. 1995;332(10):621-628.
- Sumithran P, Prendergast LA, Delbridge E, et al. Long-term persistence of hormonal adaptations to weight loss. N Engl J Med. 2011;365(17):1597-1604.
- Speakman JR, Levitsky DA, Allison DB, et al. Set points, settling points and some alternative models. Dis Model Mech. 2011;4(6):733-745.
- Sutin AR, Terracciano A. Perceived weight discrimination and obesity. PLoS One. 2013;8(7):e70048.
- Rubino F, Puhl RM, Cummings DE, et al. Joint international consensus statement for ending stigma of obesity. Nat Med. 2020;26(4):485-497.
- Marshall BJ, Warren JR. Unidentified curved bacilli in the stomach of patients with gastritis and peptic ulceration. Lancet. 1984;1(8390):1311-1315.
- World Health Organization. WHO issues its first guideline on the use of GLP-1 receptor agonists for obesity in adults. Geneva: WHO; 2025.
- Rubino F, Cummings DE, Eckel RH, et al. Definition and diagnostic criteria of clinical obesity. Lancet Diabetes Endocrinol. 2025;13(3):221-262.
Competing interests: AA is Medical Director (International) at HeliosX, which provides GLP-1 receptor agonist therapies for weight management. The views expressed are the author's own.